




Patrícia Mauro Mano
O processo natural de oxidação nada mais é do que reação entre o oxigênio obtido na respiração celular e outros elementos químicos presentes no organismo. O processo leva à perda de elétrons.1 Radicais livres, ou espécies reativas de oxigênio (ROS), são as moléculas que recebem esses elétrons livres após a reação química para formação de energia. A produção de radicais livres, não apenas é fundamental para a geração de energia, como também é essencial para o bom funcionamento do organismo.
As reações de oxidação são normalmente controladas pelo nosso corpo, que mantém o equilíbrio salutar entre a produção de radicais livres e a de compostos antioxidantes. Os antioxidantes impedem que a célula e, consequentemente, o organismo como um todo, sofra a ação maléfica das espécies reativas de oxigênio. Essas espéciesinduzem à lesão celular e, muitas vezes, à apoptose.2
Diversos motivos podem promover um desbalanço nessa equação, com consequente aumento da produção de radicais livres e menor produção de antioxidantes. Má alimentação com desnutrição celular, exposição constante a poluentes e metais pesados e a contaminação de pesticidas nos alimentos e na água são algumas delas. Quando a produção de radicais livres pelo corpo supera a produção de antioxidantes, ocorre o que chamamos de estresse oxidativo.1
O estresse oxidativo não é necessariamente maléfico ao nosso organismo. Situações como produção de massa muscular em praticantes de atividade física ou mesmo a ativação do nosso sistema imunológico necessitam de estresse oxidativo para acontecer. Consideramos o estresse oxidativo maléfico quando o seu descontrole resulta em danos aos sistemas biológicos. Assim também acontece nas disfunções do sistema vestibular.
Por meio de pesquisa no banco de dados PubMed, identificamos diversos artigos científicos que demonstram a influência do estresse oxidativo nos diferentes diagnósticos otoneurológicos.
Ohara et al1, em 2014, demonstrou que pacientes com tontura, com diferentes diagnósticos, apresentam maior produção sérica de espécies reativas de oxigênio (ROS) e menor atividade do sistema parassimpático. Tais achados desaparecem quando o sintoma é controlado.
A Tontura Postural Perceptual Persistente (TPPP), antiga tontura crônica subjetiva (TCS), é uma condição inicialmente descrita por Staab3. Sua descrição explica condições patológicas específicas de tontura persistente, não vertiginosa, que geralmente pioram com a estimulação em que possuem estimulação visual intensa ou pistas visuais conflitantes.
Estudos anteriores tentaram revelar uma causa fisiopatológica precisa para a TPPP. No entanto, a doença geralmente é causada por interações entre elementos otoneurológicos e comportamentais, dificultando seu diagnóstico para grande parte dos médicos.4 Ainda sim, a relação entre TPPP e condições psiquiátricas, como depressão, é bem estabelecidada e documentada.3
Estudos recentes do tipo metanálise correlacionam condições psiquiátricas, como a depressão, com o aumento do estresse oxidativo, ativação da micróglia e a neuroinflamaçao5. Sendo assim, é possível fazer a ponte entre a TPPP e tais achados.
Fang et al4 verificou, em um artigo publicado em 2020, o status dos componentes antioxidantes endógenos, citocinas pró-inflamatórias e a dosagem de hormônios do estresse e de serotonina em pacientes com diagnóstico de TPPP. Esses pacientes foram comparados com um grupo controle, para encontrar possíveis marcadores que auxiliassem no diagnóstico desta condição. Os autores observaram que a atividade de enzimas antioxidantes estava significativamente diminuída nesses pacientes, enquanto citocinas pró-inflamatórias, como TNF-α e IFN-γ, encontravam-se significativamente aumentadas no grupo com diagnóstico de TPPP. Os resultados demostraram ainda elevação significativa de cortisol e adrenalina, bem como redução da serotonina no grupo com TPPP em comparação ao grupo saudável. Com base nos dados, Fang et al.4 concluiu que o estresse oxidativo está envolvido na TPPP.
A doença de Ménière (DM) foi descrita pela primeira vez por Prosper Ménière em 1861. Trata-se de uma síndrome clínica caracterizada por episódios de vertigem espontâneos que duram minutos a horas, geralmente associados à perda auditiva sensorioneural flutuante, em frequências graves, associada ou não a zumbido e sensação de plenitude auditiva, em uma ou ambas as orelhas.6
A fisiopatologia da DM está associada ao acúmulo de endolinfa no ducto coclear e nos órgãos vestibulares. Embora um terço dos casos de DM possa apresentar disfunção do sistema imunológico, a resposta imune em pacientes com DM tem sido pouco investigada.6
Estados alérgicos são estados pró inflamatórios. A ligação entre alergia e DM foi descrita pela primeira vez por Duke em 19237. Em 2000, Derebery8 conduziu estudos epidemiológicos em pacientes com DM e observou que 58% dos pacientes possuíam histórico de alergia e 41% apresentaram teste cutâneo positivo.
Tanto os alérgenos inalatórios quanto alimentares têm sido associados à DM. Em um estudo não controlado, Topuz et al9 mostrou que o teste cutâneo pode induzir sintomas auditivos, como zumbido ou sensação de plenitude auditiva em 62% dos pacientes. Nesses casos, 77% dos indivíduos apresentaram aumento da pressão endolinfática medida por eletrococleografia. Os resultados do estudo sugerem que certos alérgenos podem induzir à hidropisia endolinfática.
Conforme constatado por Frejo et al.,6 quando comparados aos controles, os pacientes com DM apresentaram expressão maior de citocinas pró inflamatórias como IL-1β, TNF-α e IL-6. Em indivíduos saudáveis, os níveis de IL-1 β geralmente são indetectáveis. Nenhum dos pacientes que apresentavam citocinas pró-inflamatórias elevadas possuía infecção aguda ou outra condição autoimune que pudesse explicar essa descoberta. O autor sugere que este subconjunto de pacientes com DM e altos níveis basais de citocinas e autoanticorpos negativos pode ser considerado como portador de uma condição auto inflamatória que envolve a orelha interna. As características da doença auto inflamatória da orelha interna podem incluir uma resposta imune inata mediada por monócitos, altos níveis de IL-1β e títulos baixos/ autoanticorpos inespecíficos.6
O estudo em questão demonstrou que alguns extratos alergênicos induzem uma resposta imune pró-inflamatória na maioria dos pacientes com DM, envolvendo TNF-α, o que não é observado nos controles. Esse mecanismo poderia iniciar ou exacerbar a resposta inflamatória no saco endolinfático ou no ligamento espiral e desencadear a hidropisia endolinfática.6 Estudos anteriores também estabeleceram relação entre extratos de mofo e citocinas pró-inflamatórias na doença autoimune da orelha interna.10
Frejo et al.,6 em seu estudo, também referiu que pacientes que utilizaram imunoterapia apresentaram melhora na duração e frequência dos episódios de vertigem em comparação com os controles, e que, essa poderia ser uma alternativa de tratamento para alguns pacientes com DM.
A enxaqueca Vestibular (EV), assim como a DM, também é uma síndrome otoneurológica episódica definida por um conjunto de sintomas como vertigem, zumbido e plenitude auditiva. Tanto a EV quanto a DM podem apresentar sobreposição de sintomas e não há um marcador biológico conhecido para distingui-las. A principal diferença nos critérios de diagnóstico entre essas duas condições são os sintomas auditivos, que são necessários para o diagnóstico de DM definitiva.
Ainda sim, está relatado que pacientes com EV podem apresentar zumbido durante as crises de vertigem, e ainda que 25% dos pacientes com enxaqueca sofrem de perda auditiva. Cabe ainda lembrar que é observada uma alta prevalência de enxaqueca em pacientes com DM, sugerindo uma ligação fisiopatológica entre essas doenças.11
Flook et al,12 em 2019, se propôs a investigar o perfil de citocinas pró-inflamatórias nos pacientes com diagnóstico de DM e EV, com o objetivo de distinguir laboratorialmente essas patologias. Como já previamente descrito por Ohara1, Flook12 também observou que os controles sempre têm níveis de citocinas mais baixos do que os pacientes. Isso poderia indicar que os pacientes com MD e VM apresentam uma resposta pró-inflamatória sistêmica, justificando a resposta de alguns pacientes a medicamentos anti-inflamatórios. Por outro lado, esse aumento na produção de citocinas também poderia transparecer atividades que estão ocorrendo no interior da orelha interna. Atividades resultantes de uma resposta inflamatória prolongada que pode acarretar danos a esta estrutura por meio da ruptura do seu epitélio. Apesar de apresentar uma coorte de pacientes limitada, o autor conclui que pacientes com MD e VM possuem uma assinatura pró-inflamatória diferente e, que um painel de citocinas poderia ser usado como marcadores biológicos para o diagnóstico diferencial entre VM e MD.12
A vertigem posicional paroxística benigna (VPPB) é considerada a disfunção vestibular periférica mais comum. É caracterizada por episódios recorrentes de vertigem com duração de segundos desencadeados por movimentos da cabeça.13 O mecanismo fisiopatológico subjacente à VPPB está relacionado à presença de detritos/otólitos flutuantes no canal semicircular (canalolitíase) ou aderidos à cúpula (cupulolitíase). Acredita-se que esses otólitos se acumulem após desprendimento do neuroepitélio da mácula utricular após degeneração da estrutura, conforme aspecto observado em microscopia eletrônica. Qualquer circunstância que promova a degeneração deste epitélio parece ser capaz de causar a VPPB.14
A VPPB é considerada idiopática em cerca de 80% dos casos.13 Ainda que se aceite que o motivo do sintoma são os otólitos soltos fora de seu lugar, e que a melhora sintomática somente ocorra por meio das manobras de reposição, a pergunta que não pode deixar de ser feita é: o que gerou um processo de degeneração do epitélio macular a ponto dessas partículas se desprenderem?
Em uma revisão sistemática, Yetiser14 identificou alguns possíveis fatores associados à ocorrência de VPPB, como envelhecimento, enxaqueca, doença de Ménière, infecção, insuficiência de vitamina D, hiperglicemia e doenças autoimunes.14
Como já discutido anteriormente, o ponto em comum entre todas essas condições é o estresse oxidativo. O aumento descontrolado da formação de radicais livres causa danos endoteliais, sofrimento do neuroepitélio macular e consequente ativação de vias de sinalização apoptóticas. O desprendimento dos otólitos ocorre devido à fragilidade da superfície macular.13
Mesmo com toda a evidência que ligue os sintomas vestibulares ao estresse oxidativo, muitos estudos ainda serão necessários para nos orientar na melhor condução desses casos. Promover a limpeza ou retirada de radicais livres de nosso organismo, por meio do uso de antioxidantes exógenos, apresenta resultados limitados em comparação ao combate de sua formação, promovendo a produção de antioxidantes endógenos.
Assim, a avaliação preventiva da nutrição celular, o cuidado com o descanso e a qualidade de sono, bem como o estímulo a prática frequente de atividade física apresentam resultados promissores. Esses resultados são visíveis não apenas no controle de doenças instaladas, mas também na melhora da qualidade de vida de nossos pacientes. Esse é um campo vasto, que abre portas para uma medicina integrativa, que aborde o paciente como um todo.
Referências:
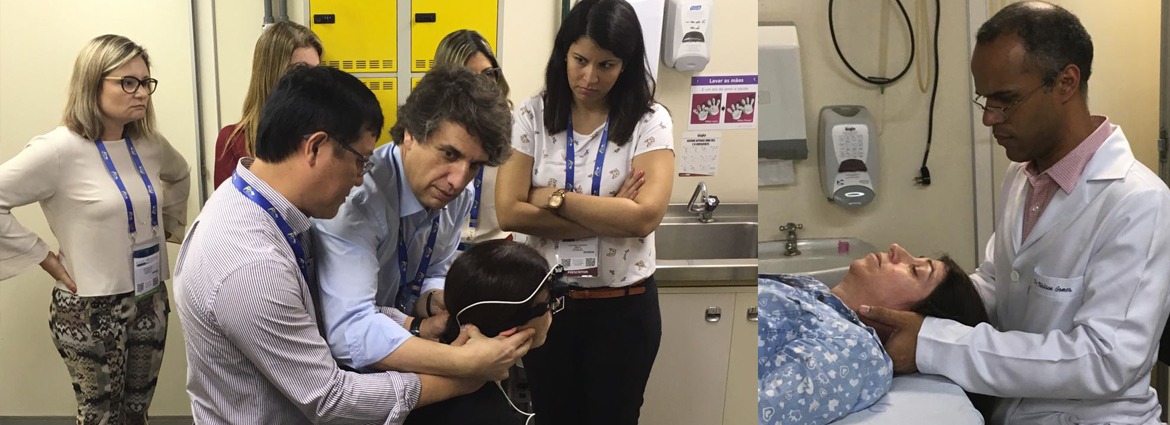
É com alegria que relatamos que o Dr Arlindo Lima, responsável pelo ambulatório de isquemias vestibulares do setor de Otoneurologia do HC-FMUSP está em visita à Coreia do Sul para aprimoramento profissional. A finalidade da visita é buscar parcerias com o Dizziness Center da Universidade Nacional de Seoul (UNS), serviço chefiado pelo Prof. Dr. Ji Soo Kim, referência mundial no assunto. O Prof Kim é respeitado e reconhecido internacionalmente por suas contribuições científicas na identificação de lesões de vias vestibulares centrais atribuídas às isquemias transitórias e acidentes vasculares cerebrais.
O intercâmbio de conhecimentos entre HC-FMUSP e UNS fomenta inovações tecnológicas e estreita ainda mais os laços do Setor de Otoneurologia do HC-FMUSP com a comunidade internacional.
Somos gratos ao Prof. Kim pela oportunidade de acompanhar seu trabalho.

Dietmar Basta 1,*, Marcos Rossi-Izquierdo 2, Kai Wonneberger 3, Cibele Brugnera 4, Roseli Saraiva Moreira Biflar 4, Mário Edvin Greters 5, Arne Ernst 1 and Andrés Soto-Varela 6
1 Department of Otolaryngology, Unfallkrankenhaus Berlin, University of Berlin, 12683 Berlin, Germany
2 Department of Otolaryngology, University Hospital Lucus Augusti, 27003 Lugo, Spain
3 Center for Otolaryngology, 47829 Krefeld, Germany
4 Department of Otolaryngology, Faculdade de Medicina FMUSP, Universidade de Sao Paulo, Sao Paulo 01246-903, Brazil
5 Department of Otolaryngology, Pontifícia Universidade Católica de Campinas, Campinas 13034-685, Brazil
6 Department of Otolaryngology, Complexo Hospitalario Universitario de Santiago de Compostela, 15706 Santiago de Compostela, Spain
* Correspondence: dietmar.basta@ukb.de
Citation: Basta, D.; Rossi-Izquierdo, M.; Wonneberger, K.; Brugnera, C.; Bittar, R.S.M.; Greters, M.E.; Ernst, A.; Soto-Varela, A. Individualized Vibrotactile Neurofeedback Training in Patients with Chronic Bilateral
Abstract: Patients with bilateral vestibulopathy (BVP) suffer from postural imbalance during daily life conditions, which in turn leads to a high frequency of falls. Unfortunately, vestibular rehabilita- tion has only modest and somewhat inconsistent effects in this patient group. Approximately 50% of BVP patients show an improved postural control after conventional vestibular rehabilitation training. New and more promising approaches are required. The individualized vibrotactile neu- rofeedback training (IVNT) in stance and gait conditions has already been described as highly ef- fective in patients with various vestibular disorders. The purpose of the present multicenter study was to determine the efficacy of the IVNT in improving balance, reducing self-perceived disability, and improving gait in patients with confirmed BVP. In total, 22 patients performed the IVNT with the Vertiguard® system for 10 daily sessions. The dizziness handicap inventory (DHI), the stance stability score of the sensory organization test (SOT) and the score for everyday life mobility in stance and gait tasks (SBDT) were obtained immediately before and after the rehabilitation training period, as well as 3 and 12 months later. All measures improved significantly after the IVNT. Be- tween 77.3% and 94.4% of patients showed an individual benefit (depending on outcome measure). The effect was not significantly reduced within the follow-up period of 12 months. The results demonstrate a high efficacy of the IVNT for vestibular rehabilitation in BVP patients.
Keywords: postural imbalance; bilateral vestibulopathy; vibrotactile neurofeedback
Vestibulopathy. Brain Sci. 2023, 13,
Received: 6 July 2023
Revised: 14 August 2023
Accepted: 15 August 2023
Published: 18 August 2023
Copyright: © 2023 by the authors. Licensee MDPI, Basel, Swiderland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/license s/by/4.0/)
Bilateral vestibulopathy (BVP) is an epidemiologically rare disease. It occurs in ap- proximately 28 of 100.000 people [1]. However, the prevalence increases with increasing age (9% in ≥65 years, 12% in ≥80 years) [2]. When those patients have subjective, clinically relevant complaints, they usually suffer from postural imbalance and unsteadiness of gait during daily life conditions that worsens in darkness and on uneven ground. This in turn leads to a high frequency of falls. A recent study reported that 43% of BVP patients expe- rienced at least one fall within a 6-month period and 70% of them were recurrent fallers [3]. The percentage of falls in patients with BVP is significantly higher than in individuals with unilateral vestibular dysfunction [4]. Whilst 83% of patients with an uncompensated unilateral vestibulopathy (UVP) feel off-balance or unsteady, 58% of UVP patients have difficulty walking in the dark, 25% have difficulties walking on uneven surfaces, 8% have blurred vision when moving their head and 8% drift to the side when trying to walk straight, all these complaints occur in 100% of BVP patients [1]. There are typically no symptoms while sitting or lying under static conditions. Some patients also complain of oscillopsia while walking. The etiology of BVP remains largely unclear in about 50% of patients (“idiopathic”). Frequent known causes are ototoxicity (e.g., due to gentamicin) [5], bilateral Menière’s disease, autoimmune disorders, meningitis and bilateral vestibular schwannoma, as well as a combination with cerebellar degeneration (cerebellar ataxia, neuropathy, vestibular areflexia syndrome (CANVAS)) [6]. Unfortunately, in the long term, there is no improvement in vestibular function and there is currently no established causal medical treatment. The recent mainstay of treatment for patients with BVP is ves- tibular rehabilitation, which relies on central compensation and the reweighting of other sensory inputs [7]. Vestibular rehabilitation has been shown to be effective for numerous vestibular disorders but is less efficacious in BVP patients [8]. Vestibular rehabilitation has only modest and somewhat inconsistent effects on postural control in this patient group [9]. Approximately 50% of BVP patients show an improved postural control after conven- tional vestibular rehabilitation training [10,11]. There is only moderate evidence that adults with BVP improve their gait and postural stability following exercise-based vestib- ular rehabilitation [12]. In particular, no significant effect was found on gait speed [10,13]. This is especially important since gait speed strongly correlates with the risk of falls. It was suggested that the benefits of physical therapy are less substantial in BVP patients than in patients with other vestibular disorders because of multiple comorbidities and a slow progression in the severity of the vestibular loss [1]. Thus, the efficacy of vestibular rehabilitation in BVP patients requires improvement. There is some evidence for an in- creased efficiency of conventional rehabilitation, if combined with the continuous appli- cation of a noisy electrical (galvanic) stimulation (nGVS), in patients with a bilateral ves- tibular loss [14]. Improvements in postural control after vestibular rehabilitation tasks with nGVS may be due to an increased information throughput within the vestibular sys- tem, due to stochastic resonance.
Vestibular rehabilitation has the primary aim of promoting central compensation and, thus, improving balance function. The central compensation of vestibular deficits is essentially a physiological process, re-evaluating remaining, nonimpaired, or nonvestib- ular stimuli (e.g., the postural muscles, vision and proprioception) to maintain balance. Most rehabilitation programs should be started as early as possible and should include feedback mechanisms to speed up the adaptation and sensory substitution of the impaired vestibular function. The approach of vibrotactile neurofeedback training is to ensure nor- mal posture or balance even with reduced vestibular, visual or proprioceptive input, by conveying the missing information through tactile stimulation. The vibro-tactile sense is particularly well suited to this, as it is processed intuitively and leads to an involuntary correction of posture. Furthermore, the vibrotactile stimulus, in contrast to the visual or acoustic stimulus, does not impede the acquisition of information from the environment. There are two different approaches in general: one with a permanent vibration signal de- pending on the body sway and a second with a signal-like stimulation only when specific swaying ranges are exceeded. The first variant is implemented, for example, by a system (BalanceBelt®) that is recommended for permanent wear instead of vestibular rehabilita- tion training. Another system (VibroTactile®) uses signal stimulation only if specific fluc- tuation values are exceeded. These thresholds are specific to each direction of body sway and should be set by a therapist. The vibratory stimulation is applied on the waist. This system is only applicable during stance tasks on a force platform. The sway is calculated based on pressure measurements on the sole of the foot. In general, the vestibular rehabil- itation protocols should be individualized to provide the best possible outcome for the patients. The latest update of the Cochran Database of Systematic Reviews indicates that moderate to strong evidence exists to support vestibular rehabilitation training being ap- plied effectively for patients with unilateral peripheral vestibular dysfunction, with the highest evidence for individualized vibrotactile neurofeedback training (IVNT) in stance and gait tasks [15].
IVNT is an approach to improve and speed up vestibular rehabilitation in stance and gait conditions, which has already been described as highly effective in patients with var- ious vestibular disorders in randomized placebo-controlled double-blind studies. In pa- tients with multifactorial dizziness in old age, uncompensated unilateral vestibulopathies and in Parkinson’s patients, a significant reduction in body swaying and the risk of falls has been demonstrated [16–19]. The single device with vibratory feedback, which could be used for IVNT in stance and gait tasks, is currently the Vertiguard®-system. The feed- back thresholds are set by the system itself based on the patient’s age and sex, and the specific sensorimotor training condition.
Before the actual training, the patient completes a body sway analysis in everyday situations, with the body swaying being continuously measured close to the body’s center of gravity. This makes it possible to objectively identify and quantify the individual defi- cits in terms of the patient’s postural control. In the subsequent training, the patient should reduce the body sway in the conditions that are problematic with the help of the additional vibrotactile signal and thus improve the body balance in everyday life.
The purpose of the present multicenter study was to determine the efficacy of the individualized vibrotactile neurofeedback training (IVNT) in improving balance, reduc- ing self-perceived disability, and improving gait in patients with confirmed BVP.
Brain Sci. 2023, 13, 1219. https://doi.org/10.3390/brainsci13081219 www.mdpi.com/journal/brainsci
All patients included in this study reported dizziness and instability under daily life conditions. The total study sample included 22 participants who had chronic, uncompen- sated bilateral vestibulopathy. Ten female and twelve male patients with a mean age of 67.4 ± 11.3 years participated in the study.
Vestibular testing included caloric testing (horizontal semicircular canal function), recording of cervical vestibular evoked myogenic potentials (cVEMP, saccular function), and analysis of subjective visual vertical (SVV, utricular function). Diagnosis of BVP was based on the slow-phase velocity of eye nystagmus (less than 6°/s during bithermal (44 °C and 30 °C) caloric irrigation) [20]. Absent cVEMP responses were found in 40.9% and path- ologic SVV-results in 27.3% of the patients. None of the participants showed severe non- vestibular sensory deficits (e.g., polyneuropathy), an acute vestibular disorder, or medi- cation that would actively influence the vestibular system (e.g., antivertiginosa). No other treatment was provided for balance disorders during the study period.
Interventions
Individualization of the rehabilitation program was based on a body sway analysis (mobile posturography) using the diagnostic function of the VertiGuard®-system (Zeisberg GmbH, Medingen, Germany). The device was mounted with a belt at the upper pelvis (iliac crest), close to the center of mass (Figure 1). Patients younger than 60 years performed the standard balance deficit test (SBDT). All other patients performed the ger- iatric standard balance deficit test (gSBDT). Both tests contain a set of 14 different every- day life stance and gait conditions [16,21]. The following tasks are included in the SBDT:
The tasks “standing on one leg with eyes closed” and “standing on one leg on a foam support surface” were substituted by “stand up” and “sit down” in the gSBDT.
For all stance tasks, the measurement time was 20 s and as long as required for gait tasks. The results of the body sway analysis were compared with age- and sex-related normative values. The normative values are inbuilt in the VertiGuard®-system and were published previously [21]. The individualized training program for vestibular rehabilita- tion consisted of up to six SBDT/gSBDT tasks which showed the largest positive difference from the normative values [16].
Individualized training was performed daily under supervision over 2 weeks, result- ing in 10 sessions as the weekend was excluded. The feedback (rehab) mode of the Verti- Guard®-system was used for the training. A training session consisted of five repetitions of each selected training task. Each repetition took a maximum of 20 s. During training, participants received a vibrotactile feedback signal for those directions that showed a higher body sway than preset individual thresholds. The preset threshold for each train- ing task was related to the age and sex of the patient and could be modified in a limited range to adjust the feedback on the participant’s daily training performance. No vibrotac- tile feedback was applied if the participant’s sway was below a preset threshold.

Figure 1. Positioning of the VertiGuard®–system close to the center of body mass for posturography and vibrotactile vestibular rehabilitation. Four vibratory actuators (front, back, left and right) are placed on the belt together with the main device.
Outcome Measures
The primary outcome measure was the Dizziness Handicap Inventory (DHI) ques- tionnaire [22]. This questionnaire characterizes disabilities resulting from balance impair- ment, with scores ranging between 0 and 100. The maximum score represents the greatest disability. The DHI and all other outcome measures were obtained immediately before and after the rehabilitation training period, as well as 3 and 12 months later.
One secondary outcome measure was the SBDT/gSBDT composite score recorded without any feedback signal. The SBDT/gSBDT composite score, a risk-of-falling indica- tor, was calculated as the sum of ratios of all SBDT/gSBDT task scores to their age- and sex-related normative values in anterior/posterior and lateral directions. It was calculated by using the following formula:
with: SBDT/gSBDTcomposite score =(∑i 𝑝i + ∑i 𝑟i) · 100
𝑘 · 400
p = pitch sway divided by normal value in %.
r = roll sway divided by normal value in %.
n = number of tasks in the SBDT or gSBDT.
This score is scaled between 0 and 100, where 100 represents the highest risk of falling and thus represents the lowest stability [21].
Furthermore, participants underwent the sensory organization test (SOT) on the an- kle-sway referenced platform BalanceMaster® (Nicolet Biomedical®, Clackamas, OR, USA), as an additional secondary outcome measure for stance stability under different sensorimotor conditions. Measurements were taken during three repeated 20 s runs under six sensorimotor standing conditions [23]. The following stance tasks were performed in the SOT: standing with eyes open/closed, standing with a moving surrounding, standing on a tilting platform with eyes open/closed, standing on a tilting platform with a moving surrounding. The SOT composite score is scored between 0 and 100, with the highest score indicating maximal stability.
Statistical Analysis
Pre- and post-training values of all outcome measures were compared using the t– test for dependent samples if they were normally distributed, whereas for non-normally distributed data, the Wilcoxon’s test was used. The Kolmogorov–Smirnov test was chosen for testing the data distribution. The level for significance of all tests was a p value less than 0.05. A similar procedure was applied for the data analysis of follow-up results. Since not all patients showed up for follow-up measures, the comparisons (pre, post, 3 months, 12 months) were only performed with results from patients who participated on all visits. A Bonferroni alpha-correction was applied for multiple comparisons.
A clinically relevant change could be surely assumed if the SBDT- or SOT-score in- creased or decreased by 10 points [21,23] or the DHI-score increased or decreased by 18 points [24], since these values are the largest differences between qualitative interpreta- tions.
Objective parameters such as SBDT and SOT scores, as well as subjective parameters such as DHI scores, were calculated before and after the training period (Figure 2).
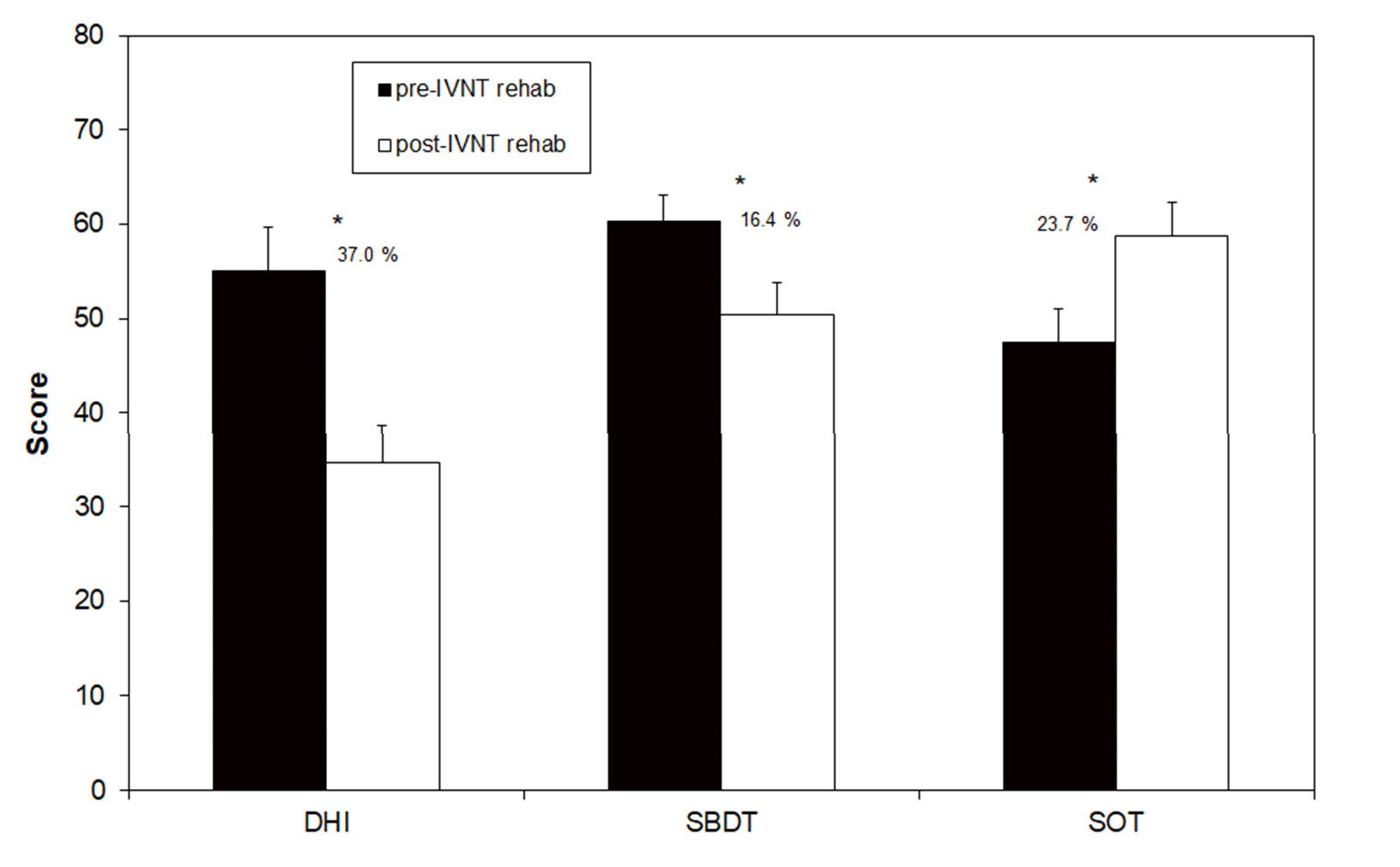
Figure 2. Scores of the Dizziness Handicap Inventory (DHI), the Standard Balance Deficit Test (SBDT) and the Sensory Organization Test (SOT) before and after the individualized vibrotactile neurofeedback training (IVNT). Asterisks indicate a significant difference between pre- and post- rehab values.
The SBDT composite score before the training was 60.3 (±3.5), which decreased to 50.4 (±3.6) after the training. This improvement of 16.4% was statistically significant and17 out of 22 patients showed a reduction in the score. A significant improvement in the SOT composite score was found when comparing pre- and post-training results: 47.5 (±2.8) and 58.8 (±3.5), respectively. The percentage increase in stance stability was 23.7%. Only one tested patient showed no improvement. DHI scores following the training were de- creased: 55.1 (±4.6) pre-training to 34.7 (±4.0) post-training, with this change representing a statistically significant improvement of 37% (Figure 2). In total, 19 out of 22 patients showed a reduction in this primary outcome measure due to the IVNT. Only three patients showed nearly no change in the DHI-score after the training (Table 1).
Table 1. Individual scores of the Dizziness Handicap Inventory before and after the individualized vibrotactile neurofeedback training (IVNT) and the related difference (post- minus pre-scores).
| Patient | DHI Pre-IVNT | DHI Post-IVNT | Delta DHI Post-Pre |
| 1 | 70 | 44 | −26 |
| 2 | 96 | 76 | −20 |
| 3 | 72 | 62 | −10 |
| 4 | 28 | 36 | 8 |
| 5 | 22 | 24 | 2 |
| 6 | 52 | 28 | −24 |
| 7 | 76 | 26 | −50 |
| 8 | 74 | 24 | −50 |
| 9 | 24 | 12 | −12 |
| 10 | 64 | 28 | −36 |
| 11 | 42 | 22 | −20 |
| 12 | 26 | 14 | −12 |
| 13 | 54 | 41 | −13 |
| 14 | 42 | 16 | −26 |
| 15 | 28 | 24 | −4 |
| 16 | 58 | 40 | −18 |
| 17 | 62 | 16 | −46 |
| 18 | 52 | 18 | −34 |
| 19 | 72 | 60 | −12 |
| 20 | 64 | 68 | 4 |
| 21 | 42 | 28 | −14 |
| 22 | 92 | 56 | −36 |
Follow-Up
Only ten patients participated in the 3- and 12-month visits. The data of all visits were analyzed for these patients separately (Figure 3). The SBDT composite score significantly decreased from 73.5 (±6.5) to 61.3 (±9.2) after the training (16.6% change) and remained stable during the next 12 months (62.5 ± 8.8 after 3 months and 63.0 ± 9.7 after 12 months). The SOT-score also showed a significant change from 38.2 ± 3.3 to 49.5 ± 4.9 after the training (22.9% change). There was a clear but not significant reduction in the score 3 and 12 months after the training (39.7 ± 4.0 after 3 months and 43.3 ± 4.2 after 12 months).
The DHI-score was not significantly changed, if compared before and after the train- ing (49.7 ± 8.9 before and 43.7 ± 7.3 after the training), after the training and 3 months later (40.7 ± 9.1) and between the next 9 months of the follow-up (38.7 ± 7.4). There was a sta- tistically significant decrease in the DHI-score by 22.1% between the pre-training values and the 12-month follow-up (Figure 3).
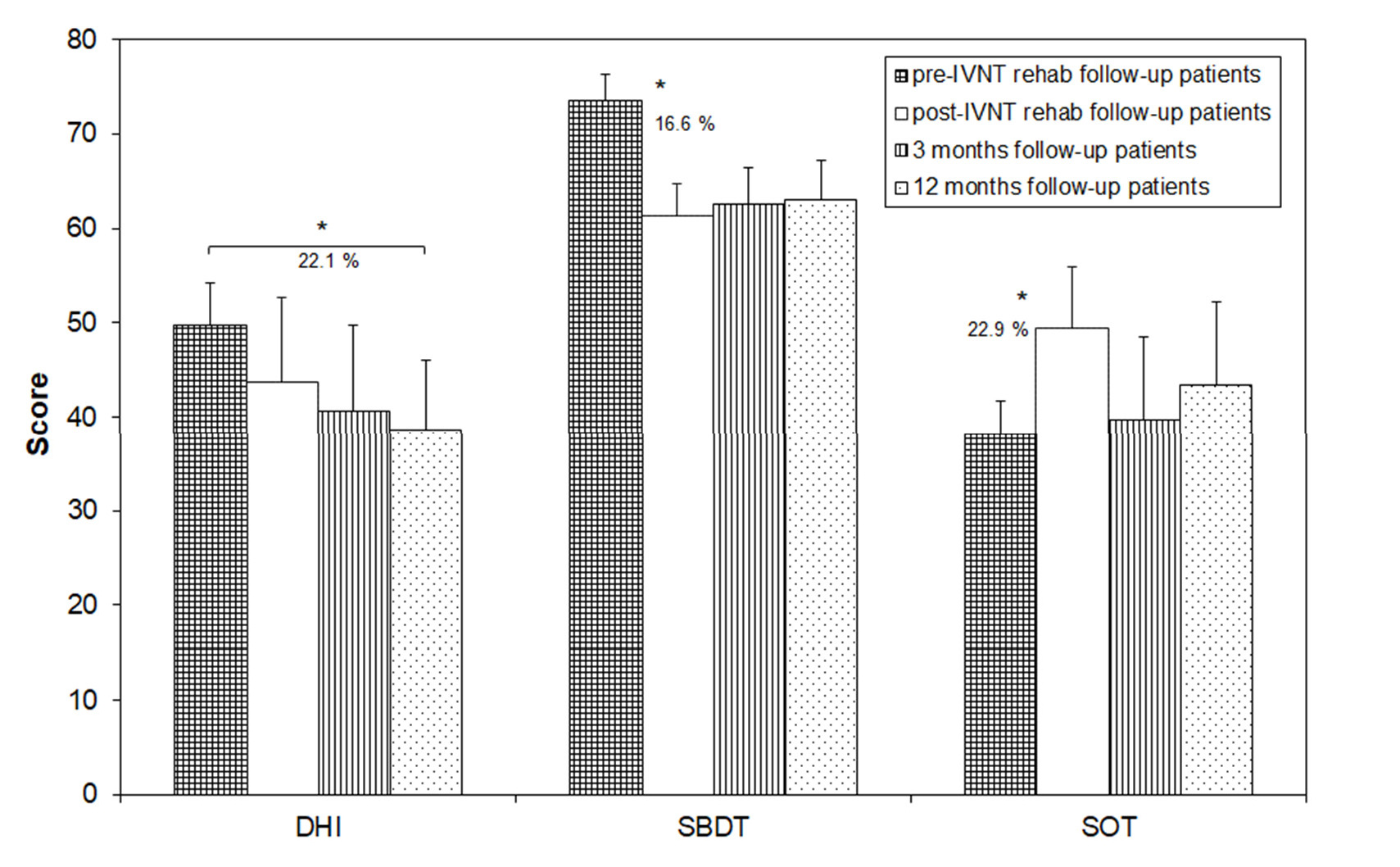
Figure 3. Scores of the Dizziness Handicap Inventory (DHI), the Standard Balance Deficit Test (SBDT) and the Sensory Organization Test (SOT) in patients which showed-up for the follow-up measures before and after the individualized vibrotactile neurofeedback training (IVNT) as well as 3 and 12 months later. Asterisks indicate a significant difference between the time points.
A vestibular rehabilitation by IVNT over 10 days was able to significantly enhance the objectively determined postural control during stance and gait tasks. These improve- ments were found in both objective methods: the ankle sway referenced platform system and the sway measurement close to the center of gravity. Interestingly, not only significant group improvements were found. A total of 77.3% of all patients enhanced their postural
control on an individual basis during everyday life stance and gait tasks and 94.4% during different sensorimotor stance tasks. These values are much more pronounced than earlier reported for any other vestibular rehabilitation in BVP patients. Gillespie and Minor (1999) [10] reported 51% of patients showed improvement after a conventional vestibular rehabilitation and Herdmann et al. (2015) [9] reported between 38 and 86% (depending on the outcome measure). Interestingly, the latter study showed the highest success rate in functional tests (e.g., gait speed, dynamic visual acuity) and the lowest success rate in subjective scores. However, the increased stability of the patients in the present study was also reflected by a significant decrease in the subjectively reported dizziness handicap. This holds true as a group measure as well as on an individual basis. An individual de- crease in the DHI-score was observed in 86.4% of all treated patients. This is a higher rate of improvement compared to other studies. A recent study, which combined conventional vestibular training with noisy galvanic vestibular stimulation for treatment of bilateral vestibulopathy, failed to show a decrease in the DHI group value, even if the postural stability during stance tasks could be significantly improved [25]. Brown et al. (2001) [11] differentiated between the percentage of patients with a DHI improvement and the per- centage of patients with a clinically significant change in the DHI score. The minimal clin- ically significant change was defined as a change of 18 points. Unfortunately, the back- ground of this cut-off value was not further explained but is possibly related to the largest difference between qualitative interpretations [24]. Based on this criterion, 33% of all pa- tients in the study of Brown et al. (2001) [11] showed a clinically significant change of the DHI scores. In the present study, the rate of improvement as calculated due to Brown et al. (2001) [11] was 54%. This evidently demonstrates the superior efficacy of the IVNT as vestibular rehabilitation measure in BVP patients.
The follow-ups could only be performed in nearly half of the patients. These patients showed no significant group improvement in the subjective measure (DHI) directly after the training and 3 months later. Possibly, this is why they participated in the follow-up visits. The phenomenon, that mainly patients with subjective poor improvement show up for follow-up visits is well documented [16]. Surprisingly, these patients enhanced their objectively measured postural control in the present study directly after the IVNT. A sig- nificant increase of the subjective improvement was only found 12 months after the train- ing, even if the objective measures for postural control were nearly unchanged or not sig- nificantly worse meanwhile. These opposite results are possibly related to the patients’ expectations. The postural control was lower in these patients before the training, if com- pared to the entire group, and the improvement directly after the training was “only” similar. Since the DHI-scoring is not linearly related to the patient´s handicap (DHI; 16– 34 points = mild handicap, 36–52 points = moderate handicap, >54 points = severe handi- cap) [24], the next step of improved handicap perception was possibly not fulfilled directly after the training.
Anyway, all follow-up measures improved after the IVNT for at least 12 months, which would suggest that such a long-term effect is not directly related to the IVNT train- ing alone. The patients were probably mobilized and left their sedentary lifestyle since they were better able to maintain postural control during any physical activity. Thus, en- hanced physical activity should have contributed to the reported long-term benefit as well.
One limitation of the study is the lack of a control group. Adding a control group is always difficult in a study that investigates a rare disease. This was also shown in previous studies by the very limited numbers of patients in the experimental group and the controls (mainly below 10) [12]. This is a disadvantage for the statistical power of the study. How- ever, the absolute lack of any effect of a placebo application in the IVNT method (only performing the exercises without the vibrotactile stimuli) was already shown for a couple of other vestibular disorders [16]. Even if similar results are expected for BVP patients, future larger studies should include a control group (e.g., placebo).
The results of the current study show that BVP patients can be effectively rehabili- tated with the easy to perform IVNT method in stance and gait conditions. This holds true not only for the whole investigated sample, but also for almost all individual patients. One limitation of the method is that the patient should be able to perform at least some of the tasks included in the SBDT/gSBDT. This is analyzed by the body sway analysis, which always precedes the rehabilitation training.
Furthermore, there is some evidence that the single 10-day training could have a long-term effect that lasts at least 12 months. However, this should be further investigated in a larger sample of BVP patients with a clear record of individual physical activity.
Author Contributions: Conceptualization, D.B., A.E. and A.S.-V.; methodology, D.B. and A.S.-V.; validation, A.S.-V., M.R.-I. and R.S.M.B.; formal analysis, M.E.G. and D.B.; investigation, C.B., M.R.- I., D.B., A.S.-V. and K.W.; writing—original draft preparation, D.B.; writing—review and editing, A.E., M.R.-I., A.S.-V., C.B., K.W. and R.S.M.B.; visualization, D.B.; supervision, A.E.; project admin- istration, D.B. All authors have read and agreed to the published version of the manuscript.
Funding: This research received no external funding.
Institutional Review Board Statement: The Institutional Review Board approved the study proto- col (EA1/134/09) and the study was conducted in accordance with the Declaration of Helsinki on Ethical Principles for Medical Research Involving Human Subjects.
Informed Consent Statement: Informed consent was obtained from all subjects involved in the study.
Data Availability Statement: All data are available upon request from the corresponding author.
Conflicts of Interest: The authors declare no conflicts of interest.
| 1. Ward, B.K.; Agrawal, Y.; Hoffman, H.J.; Carey, J.P.; Della Santina, C.C. Prevalence and impact of bilateral vestibular hypofunc- tion: Results from the 2008 US National Health Interview Survey. JAMA Otolaryngol. Head Neck Surg. 2013, 139, 803–810. |
| 2. Piper, K.S.; Juhl, C.B.; Andersen, H.E.; Christensen, J.; Søndergaard, K. Prevalence of bilateral vestibulopathy among older adults above 65 years on the indication of vestibular impairment and the association with Dynamic Gait Index and Dizziness Handicap Inventory. Disabil. Rehabil. 2023, 45, 1220–1228. |
| 3. Wuehr, M.; Decker, J.; Schenkel, F.; Jahn, K.; Schniepp, R. Impact on daily mobility and risk of falling in bilateral vestibulopathy. J. Neurol. 2022, 269, 5746–5754. |
| 4. Herdman, S.J.; Blatt, P.; Schubert, M.C.; Tusa, R.J. Falls in patients with vestibular deficits. Am. J. Otol. 2000, 21, 847–851. |
| 5. Skarzynska, M.B.; Król, B.; Czajka, L. Ototoxicity as a side-effect of drugs: Literature review. J. Hear Sci. 2020, 10, 9–19. |
| 6. Kim, J.S.; Kim, H.J. Bilateral vestibulopathy: The causes, diagnosis, and treatments. Curr. Opin. Neurol. 2022, 35, 98–106. |
| 7. Medendorp, W.P.; Alberts, B.B.G.T.; Verhagen, W.I.M.; Koppen, M.; Selen, L.P.J. Psychophysical Evaluation of Sensory Re- weighting in Bilateral Vestibulopathy. Front. Neurol. 2018, 25, 377. |
| 8. Telian, S.A.; Shepard, N.T.; Smith-Wheelock, M.; Hoberg, M. Bilateral vestibular paresis: Diagnosis and treatment. Otolaryngol. Head Neck Surg. 1991, 104, 67–71. |
| 9. Herdman, S.J.; Hall, C.D.; Maloney, B.; Knight, S.; Ebert, M.; Lowe, J. Variables associated with outcome in patients with bilateral vestibular hypofunction: Preliminary study. J. Vestib. Res. 2015, 25, 185–194. |
| 10. Gillespie, M.B.; Minor, L.B. Prognosis in bilateral vestibular hypofunction. Laryngoscope 1999, 109, 35–41. |
| 11. Brown, K.E.; Whitney, S.L.; Wrisley, D.M.; Furman, J.M. Physical Therapy outcome for persons with bilateral vestibular loss. Laryngoscope 2001, 111, 1812–1817. |
| 12. Porciuncula, F.; Johnson, C.C.; Glickman, L.B. The effect of vestibular rehabilitation on adults with bilateral vestibular hypo- function: A systematic review. J. Vestib. Res. 2012, 22, 283–298. |
| 13. Krebs, D.E.; Gill-Body, K.M.; Parker, S.W.; Ramirez, J.V.; Wernick-Robinson, M. Vestibular rehabilitation: Useful but not univer- sally so. Otolaryngol. Head Neck Surg. 2003, 128, 240–250. |
| 14. McLaren, R.; Smith, P.F.; Taylor, R.L.; Ravindran, S.; Rashid, U.; Taylor, D. Efficacy of nGVS to improve postural stability in people with bilateral vestibulopathy: A systematic review and meta-analysis. Front. Neurosci. 2022, 16, 1010239. |
| 15. McDonnell, M.N.; Hillier, S.L. Vestibular rehabilitation for unilateral peripheral vestibular dysfunction. Cochrane Database Syst. Rev. 2015, 13, CD005397. |
| 16. Basta, D.; Rossi-Izquierdo, M.; Soto-Varela, A.; Greters, M.E.; Bittar, R.S.; Steinhagen-Thiessen, E.; Eckardt, R.; Harada, T.; Goto, F.; Ogawa, K.; et al. Efficacy of a vibrotactile neurofeedback training in stance and gait conditions for the treatment of balance deficits -a double-blinded, placebo-controlled multicenter study. Otol. Neurotol. 2011, 32, 1492–1499. |
| 17. Rossi-Izquierdo, M.; Ernst, A.; Soto-Varela, A.; Santos-Pérez, S.; Faraldo-García, A.; Sesar-Ignacio, A.; Basta, D. Vibrotactile neu- rofeedback balance training in patients with Parkinson’s disease: Reducing the number of falls. Gait Posture 2013, 37, 195–200. |
| 18. Brugnera, C.; Bittar, R.S.M.; Greters, M.E.; Basta, D. Effects of vibrotactile vestibular substitution on vestibular rehabilitation— Preliminary study. Brazil. J. Otolaryngol. 2015, 81, 616–621. |
| 19. Soto-Varela, A.; Rossi-Izquierdo, M.; Del-Río-Valeiras, M.; Faraldo-García, A.; Vaamonde-Sánchez-Andrade, I.; Lirola-Delgado, A.; Santos-Pérez, S. Vestibular rehabilitation with mobile posturography as a “low-cost” alternative to vestibular rehabilitation with computerized dynamic posturography, in old people with imbalance: A randomized clinical trial. Aging Clin. Exp. Res. 2021, 33, 2807–2819. |
| 20. Strupp, M.; Kim, J.S.; Murofushi, T.; Straumann, D.; Jen, J.C.; Rosengren, S.M.; Della Santina, C.C.; Kingma, H. Bilateral ves- tibulopathy: Diagnostic criteria Consensus document of the Classification Committee of the Bárány Society. J. Vestib. Res. 2017, 27, 177–189. |
| 21. Basta, D.; Rossi-Izquierdo, M.; Soto-Varela, A.; Ernst, A. Mobile posturography: Posturographic analysis of daily-life mobility. Otol. Neurotol. 2013, 34, 288–297. |
| 22. Kurre, A.; van Gool, C.J.; Bastiaenen, C.H.; Gloor-Juzi, T.; Straumann, D.; de Bruin, E.D. Translation, cross-cultural adaptation and reliability of the German version of the dizziness handicap inventory. Otol. Neurotol. 2009, 30, 359–367. |
| 23. Nashner, L.M. Computerized Dynamic Posturography. In: Practical Management of the Dizzy Patient; Goebel, J.A., Ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2001; pp. 143–170. |
| 24. Jahn, K.; Saul, A.K.; Elstner, M.; Sapa, K.; Kellerer, S. Vestibular rehabilitation therapy and Nintendo Wii balance board training both improve postural control in bilateral vestibulopathy. J. Neurol. 2018, 265, 70–73. |
| 25. Eder, J.; Kellerer, S.; Amberger, T.; Keywan, A.; Dlugaiczyk, J.; Wuehr, M.; Jahn, K. Combining vestibular rehabilitation with noisy galvanic vestibular stimulation for treatment of bilateral vestibulopathy. J. Neurol. 2022, 269, 5731–5737. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual au- thor(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content.
Dr Rodrigo Guizardi
Disciplina de ORL da Faculdade de Medicina da Universidade de Marília – SP
A Barreira Hematolabiríntica (BHL), assim como a Barreira Hematoencefálica (BHE), é uma estrutura fundamental para homeostase da orelha interna/SNC e já amplamente pesquisada na medicina moderna. É uma interface entre os órgãos periféricos e o SNC e controla seletivamente a troca de substâncias entre eles, mantendo o equilíbrio bioquímico e fisiológico no ambiente intersticial e celular.
Os principais atores das BHL e BHE são as células e junções endoteliais compactas que revestem os vasos sanguíneos e permitem apenas a passagem de pequenas moléculas lipossolúveis, gases e íons. Outras moléculas maiores, como a glicose, dependem de canais específicos. Portanto fica clara a importância dessas barreiras para adequada fisiologia dos fluídos, íons, moléculas e do equilíbrio oxidativo das vias auditivas e labirínticas.
Classicamente, as doenças da orelha interna, como Meniere, VPPB, neurites e perdas auditivas, são amplamente estudadas como entidades distintas, seus respectivos mecanismos fisiopatológicos, fatores de risco e opções terapêuticas. A análise atenta desses estudos e de vasta literatura sobre fisiologia, bioquímica e bases fisiopatológicas das doenças crônicas que acometem o corpo humano, demonstra um ponto convergente entre todas elas: a inflamação crônica estéril, também denominada inflamação crônica de baixo grau.
Caracteristicamente essa inflamação apresenta um curso longo, por vezes silencioso e com uma grande dissociação de sinais e sintomas. Por suas características, por muitas vezes a inflamação passa despercebida diante da visão médica tradicional não integrativa. A má alimentação, disbiose, o estresse com desregulação do eixo Hipotálamo-Hipófise-Adrenais, sobrepeso/obesidade, sedentarismo, tabagismo, poluição e intoxicação por metais pesados são exemplos dos grandes catalisadores do processo.
O desequilíbrio da cascata inflamatória, com a liberação persistente de citocinas inflamatórias, provoca um incremento significativo do estresse oxidativo, desorganização funcional celular, lesão tissular e do DNA. Sendo assim, é fácil entender a base fisiopatológica de múltiplas patologias que a medicina tradicional enxerga e trata como entidades distintas. Entre esses diagnósticos estão a aterosclerose, câncer, a neurodegeneração, artroses, cardiopatias, DPOC, asma, sinusite crônica, assim como as doenças otoneurológicas.
Ao revisar as publicações sobre fatores de risco relacionados a doenças da orelha interna, encontramos uma significativa quantidade de referências a distúrbios metabólicos. Entre eles a diabetes, hiperinsulinemia, tireoidopatias, dislipidemias, autoimunidade, vírus, drogas ototóxicas, ruído, SAHOS, hipovitaminoses, disbiose, etc…
A questão é: Mas afinal, há um elo comum entre todos eles?
E a resposta é: Sim! A inflamação crônica estéril/estresse oxidativo com a possível disfunção da barreira hematolabiríntica.
Revendo a literatura específica, citamos alguns estudos que sugerem a interrelação entre as doenças da orelha interna e o processo inflamatório crônico:
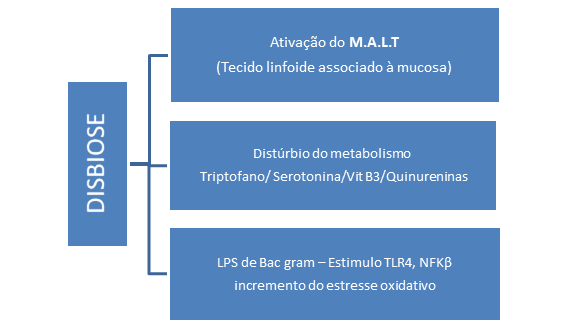
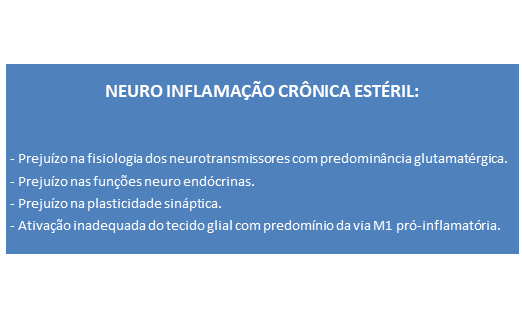
A propósito deste assunto, é de grande importância para o médico otorrinolaringologista a visão integrativa sistêmica da relação entre a disbiose, BHL e neuroinflamação crônica estéril. Essa associação pode ser observada no organograma que segue.

Uma interessante publicação do Word Journal of Otorhinolaryngology em 2013, a respeito da perda auditiva neurossensorial súbita idiopática, busca integrar as diversas hipóteses diagnósticas da perda auditiva. Em todas elas os autores encontram o “estresse” como gatilho para o desequilíbrio do sistema imunológico com a liberação de citocinas, ativação inadequada do eixo Hipotálamo-Hipósise-Adrenais e do sistema nervoso autônomo, que impactam negativamente na fisiologia coclear. Nesse caso a ativação do NFKB pode ser a via de convergência entre os “estressores sistêmicos”.
O estresse oxidativo também foi atribuído aos pacientes com VPPB, em um artigo de 2018 do The Journal of International Advanced Otology. Nesse estudo, 62 pacientes foram divididos em 2 grupos (saudáveis e VPPB) e no grupo VPPB foi observada a maior prevalência do status inflamatório, por ação direta dos radicais livres e desbalanço metabólico do cálcio. A propósito, vale a pena lembrar que os otólitos são formados por carbonato de cálcio, cujas fracas ligações são muito mais sensíveis ao estresse oxidativo e às variações de ph. Os ossos, por outro lado, são formados por fosfato de cálcio, cujas ligações mais fortes são, possivelmente, fruto evolutivo da exigência muscular.
Creio que uma melhor compreensão sobre a inflamação crônica estéril, seus gatilhos e mecanismos fisiopatológicos, que repercutem nos diversos sistemas orgânicos, trará definitivamente uma mudança de olhar do médico em relação às doenças, bem como uma fabulosa ampliação no arsenal de “ferramentas terapêuticas”.
REFERÊNCIAS BIBLIOGRÁFICAS
Abbott N. Inflammatory mediators and modulation of blood-brain barrier permeability. Cell Mol Neurobiol 2000; 20:131-147. {Google Scholar} {Cross Ref} {PubMed}.
CryanJF; DinanTG. Mind-altering microorganisms: The impacto f the gut microbiota on brain and behaviour. NatRev Neurosci 2012; 13:701-712.
Ishiyama, Gail “et al”. Estresse oxidativo no sangue. Barreira labiríntica na mácula. Utrículo de pacientes com Doença de Ménière. Frontiers in Physiology 2018, 9:1068.
Karzaki, Jin; Masuda, Masatsugu. Causa da perda auditiva neurossensorial súbita idiopática: A teoria da resposta ao estresse. Word Journal of Otorhinolaryngology 2013, Japan. 3: 42-57.
Kociszeuska, Dagmara; “et al”. A ligação entre disbiose intestinal causada por uma dieta rica em gordura e perda auditiva. Jornal Internacional de ciências ortomoleculares 2021, vol 22.
Megantara, Sacerdote. O papel da disbiose intestinal na fisiopatologia do zumbido: Uma revisão da literatura. ITJ, 2022, vol 26.
O’Mahony, S.M.; Clarke, G.; Borre, Y.E.; Dinan, T.G.; Cryan, J.F. Serotonin, tryptophan metabolismo and brain-gut-microbiome axi. Behav. Brain Res 2015, 277:32-48.
Rothhammer V, Mascanfroni ID, Bunse L, Takenaka MC, Kenison JE, Mayo L, et al. Type I interferons and microbial metabolites of tryptonphan modulate astrocyte activity and central nervous system inflamation via the hydrocarbon receptor. Nat Med 2016; 22:586-97.
Sahim, Ethem “et al”. Estado oxidatro em pacientes com vertigem posicional paroxística benigna. The Journal of Internacional Advanced Otology 2018, 14:02.
Smith R S. The macrophage theory of depression. Medical Hypotheses 1991;35(4):298-306.
Wohleb E S, McKim D B, Sheridan J F, Godbout J P. Monocyte trafficking to the brain with stress and inflammation: a novel axis of imune-to-brain communication that influences mood and behavior. Front Neurosci 2014; 8:447.
Nos dias 20 e 21 de março de 2023 aconteceu o XVII Curso de Otoneurologia Básica – princípios e práticas no Hospital das Clínicas da Faculdade de Medicina da Universidade de São Paulo. O curso teórico abordou assuntos fundamentais para a compreensão da anatomofisiologia do sistema vestibular e suas disfunções. Foram apresentadas as doenças vestibulares mais prevalentes, os exames otoneurológicos atuais e o enfoque na multidisciplinariedade necessária para a reabilitação vestibular. Novamente o curso recebeu alunos de várias regiões do Brasil e do exterior.
Durante o segundo dia do curso os alunos conheceram os diversos equipamentos utilizados no Setor de Otoneurologia. Foram discutidos o funcionamento, manuseio dos aparelhos, suas principais indicações e interpretação de seus traçados.
Agradecemos a presença de nossos alunos na XVII edição do curso.








Na data de 15/02/2023, recebemos em nosso serviço o Doutor Rodrigo Guizardi, docente da Universidade de Marília (UNIMAR), nacionalmente reconhecido por seu conhecimento da Medicina Integrativa.

Inicialmente, o Doutor Rodrigo conheceu nosso Ambulatório de Otoneurologia, acompanhando os atendimentos médicos e participando da discussão dos casos clínicos.
Após isso, nos presenteou com a aula “ Otoneurologia e Medicina Integrativa – um casamento perfeito”, onde discorreu sobre as bases da Medicina Integrativa e o papel do estresse oxidativo nas doenças otoneurológicas. Ressaltou a importância da boa anamnese, do raciocínio clínico, ampliado e integrado para melhor abordagem e seguimento adequado do paciente.
Agradecemos ao Doutor Rodrigo Guizardi, pela disponibilidade e pela oportunidade de aprendizado!

Lucas Resende L Mangia
Departamento de Otorrinolaringologia e Oftalmologia da Universidade Federal do Paraná (UFPR)
A relação entre os níveis dos hormônios sexuais femininos e o funcionamento do sistema vestibular é descrita de diferentes maneiras na literatura médica. Assim, há estudos que mensuram – tanto por meio de parâmetros da função vestibular quanto pela ocorrência de sintomas clínicos, os efeitos das flutuações do estradiol e da progesterona nas vias relacionadas ao equilíbrio e à percepção espacial. Esses estudos demonstram variabilidades de aspectos funcionais e clínicos de acordo com a fase do período menstrual.1–6
O climatério é uma fase da vida da mulher caracterizada por uma transição hormonal frequentemente acompanhada por sintomatologia diversa. Ocorre entre a vida reprodutiva e a senescência e é altamente variável em seus aspectos temporais e clínicos. Possui idade de início, duração, tipos de manifestações e intensidade muito individualizadas.
Do ponto de vista hormonal, é caracterizado por duas tendências principais. A primeira é de queda longitudinal dos níveis do estradiol e da progesterona que estarão, ao final do período, bastante reduzidos em comparação à fase reprodutiva que o antecede. A segunda é de flutuação desses índices, de maneira que a queda longitudinal não é linear nem uniforme. Apresenta, além das variações próprias do ciclo menstrual, flutuações ciclo a ciclo e de indivíduo para indivíduo (Figura 1).
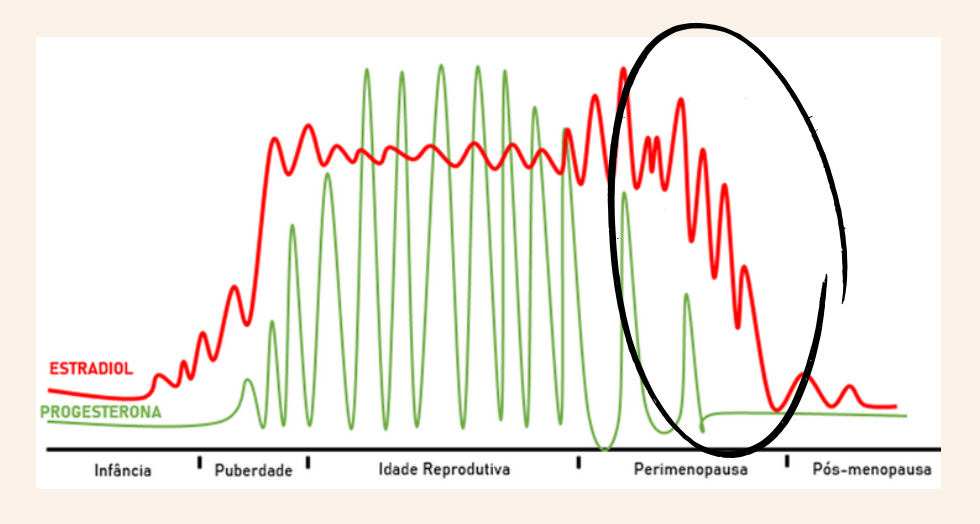
Figura 1: Esquema das tendências longitudinais dos níveis dos principais hormônios sexuais femininos ao longo da vida da mulher. No climatério, em destaque, há redução progressiva não linear dos níveis hormonais. Fonte: o Autor.
Clinicamente, a gama de sintomas relacionados ao climatério é ampla (Tabela 1) e também muito particular a cada paciente, possivelmente por representarem manifestações de vulnerabilidades individuais. Assim, a presença de ciclos irregulares e os sintomas vasomotores – tipicamente fogachos e sudorese noturna, são os mais típicos. Contudo, alterações de humor, prejuízo cognitivo, tendência ao acúmulo de gordura abdominal, piora da qualidade do sono, dores musculares e ósteo-articulares e cefaleia são também frequentemente reportados.7
| Sintomas comumente relatados no climatério | |
| Fogachos e suores noturnos | Tontura |
| Ciclos menstruais irregulares | Fadiga |
| Alterações do humor: labilidade emocional, ansiedade, nervosismo, irritabilidade. | Dores ósteo-articulares |
| Déficits cognitivos: prejuízo da atenção, lapsos de memória, perda da concentração. | Atrofia da mucosa urogenital: dispareunia, coceira vaginal, disúria |
| Ganho de peso | Palpitações |
| Insônia | Diminuição da libido |
| Dores de cabeça | |
Tabela 1: Sintomas mais comuns durante o climatério.
Sintomas vestibulares são muito prevalentes em mulheres durante a transição climatérica. Entretanto, apesar das descrições em inquéritos de até 60% de ocorrência de tonturas nesse período, trata-se de uma sintomatologia largamente negligenciada.8–10 Assim, há poucos estudos clínicos sobre o assunto e as escalas, protocolos e diretrizes direcionados ao climatério infelizmente desprezam o quadro vestibular. Pesquisas em bases de dados da literatura médica, por exemplo, retornam escassos estudos focados no tema e, aqueles existentes, lidam com o quadro vestibular de modo superficial e inespecífico. Assim, pouco se sabe até então sobre as características semiológicas da tontura relatada durante o climatério, as doenças envolvidas e suas repercussões funcionais no labirinto e vias vestibulares centrais. Por outro lado, estudos preliminares registram o impacto significativo da queixa de tontura na mulher climatérica em diferentes domínios de avaliações de qualidade de vida.11 Como resultado, tais pacientes sofrem por terem seus sintomas minimizados, ignorados ou atribuídos vagamente a quadros emocionais.
Até o momento, as bases fisiopatológicas que regem a relação entre tontura e climatério estão escassamente elucidadas. O tema é complexo, pois abarca intrincada rede de fatores possivelmente envolvidos e vieses de confusão a serem ponderados. Além disso, as informações advindas de estudos clínicos não são inequívocas e estão comumente contaminadas pela heterogeneidade das populações estudadas e dos dados coletados. Ainda, deve-se sublinhar que os estudos pecam por dissecarem superficial e insuficientemente as queixas vestibulares apresentadas pelas mulheres avaliadas – limitando a proposição de inferências sólidas no que tange o assunto.
Dessa maneira, o alicerce do conhecimento atual em relação à matéria advém de estudos eminentemente de ciências básicas, a nível celular e tecidual, que são reforçados por investigações em modelos animais. Em suma, pode-se compreender o climatério como um estado de transição neurológica em que, à semelhança da puberdade, uma série de vias regulatórias complexas do organismo da mulher são ativadas ou inativadas. Essa reorganização fisiológica, por sua vez, predispõe à manifestação de vulnerabilidades individuais de diferentes sistemas orgânicos – que resultariam, em última análise, na eclosão de sintomas e síndromes particulares a cada mulher durante o período.12
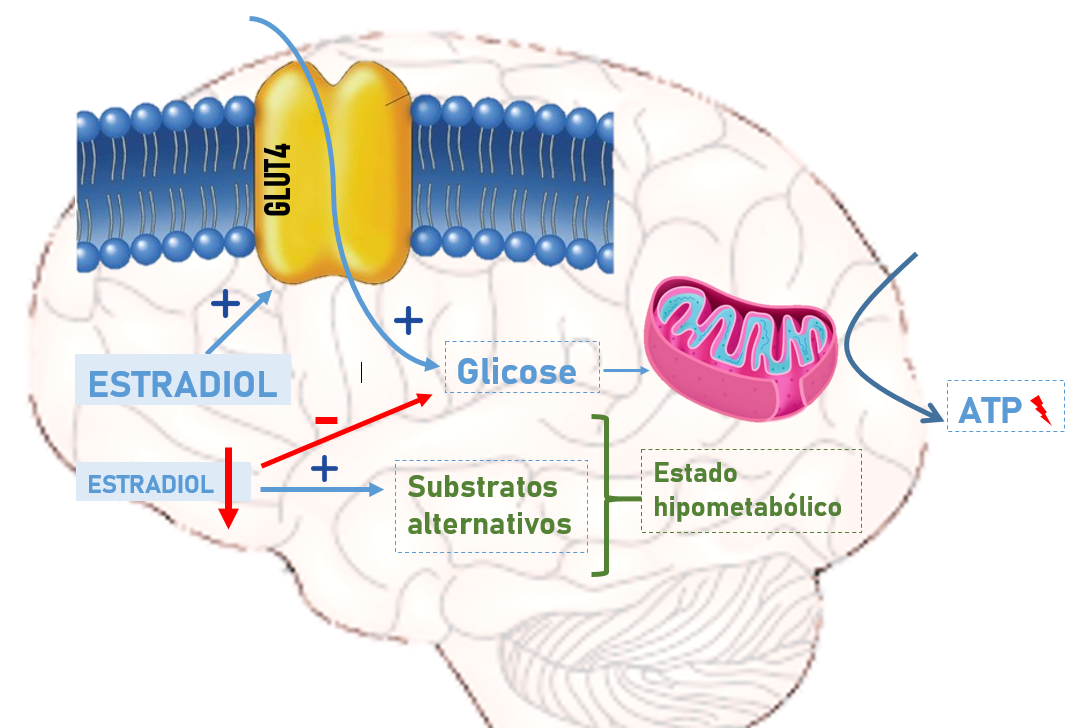
Figura 2: Esquema demonstrando os efeitos do estradiol, e consequentemente de sua redução, sobre o metabolismo energético no sistema nervoso central. Fonte: o Autor.
De maneira mais específica e sobre base científica sólida, três mecanismos principais podem ser aventados para explicar o impacto das flutuações e reduções dos hormônios sexuais femininos – em especial o estradiol, nas diversas instâncias do sistema vestibular. Em primeiro lugar: o estradiol regula o metabolismo energético celular no sistema nervoso central. Nesse tecido, a fonte de energia primária é a glicose que, transportada para o interior da célula, sofre catabolismo aeróbio para geração de energia. Sob efeito estrogênico, o transporte intracelular de glicose é otimizado e a eficiência energética da célula aumenta. Em contrapartida, diante de índices séricos reduzidos desse hormônio, o tecido nervoso passa a utilizar substratos alternativos, como ácidos graxos e corpos cetônicos, com limitação da produção de energia (Figura 2).13 Assim, pode-se considerar que a transição climatérica implicaria na emersão de um estado hipometabólico no sistema nervoso central, com possível prejuízo secundário de atividades de alta demanda, como processamento de informações complexas, integração de aferências e resposta rápida a estímulos intercorrentes. Em segundo lugar: deve ser lembrado que o estradiol – mediante ligação ao seu receptor celular, promove efeitos diversos que pendem o equilíbrio entre vias pró- e anti-inflamatórias do organismo em favor da inibição da inflamação tecidual. Esse efeito é mediado, entre outros, pela estimulação do eixo hipófise-adrenal, da produção de óxido nítrico e da formação de antioxidantes. Além disso, a função linfocitária e a produção de citocinas inflamatórias, como a interleucina 6 e o fator de necrose tumoral alfa, são coibidas.14 Consequentemente, diante dos níveis hormonais decrescentes do climatério, ocorre um estado pró-inflamatório – capaz de engatilhar ou aguçar comorbidades vestibulares diversas. Por fim: cumpre ressaltar o efeito direto e particular do estradiol no sistema vestibular e perceptual. Nesse sentido, sob ação estrogênica observa-se incentivo à plasticidade sináptica em regiões como o cerebelo e o hipocampo, sensíveis à ação desse hormônio e fundamentais na modulação da aferência labiríntica e processamento perceptual, respectivamente.15 Essa estimulação envolve a ativação celular de fatores de transcrição gênica relacionados à produção de neurotrofinas como o fator neurotrófico derivado do cérebro (BDNF, do termo em inglês).16 Uma menor densidade sináptica em vestíbulo-cerebelo concorrente à supressão estrogênica pode implicar em prejuízo da modulação reflexo vestíbulo-ocular (RVO), uma vez que esse arco reflexo é finamente ajustado por fibras de Purkinje.15
Dessa maneira, os mecanismos que podem explicar o impacto dos hormônios sexuais femininos, em especial o estrógeno, no sistema vestibular da mulher durante o climatério envolvem, resumidamente:
Ainda que incipientes, estudos clínicos também lançam luz sobre a associação entre tontura e climatério e sobre as bases fisiopatológicas dessa relação. Estudos dos sintomas climatéricos por análise de agrupamentos (clusters) colocam a tontura à parte dos sintomas vasomotores e psicológicos, assim como outras manifestações consideradas “atípicas”.17 Esse achado prenuncia uma fisiopatologia própria e muito provavelmente multifatorial para o sintoma. Por outro lado, há investigações que reforçam o vínculo da queixa vestibular com algumas queixas climatéricas, salientando possíveis elos fisiopatológicos entre elas e os efeitos dos hormônios sexuais femininos no aparato vestibular. Desse modo, o rastreio positivo de ansiedade pela escala HADS (Hospital Anxiety and Depression Scale) foi significativamente relacionado à ocorrência de tontura entre mulheres climatéricas.18 Além disso, a presença de sintomas vasomotores nessas mulheres também foi associada de maneira significativa à ocorrência de queixas de tontura e instabilidade postural e à menor taxa de recuperação após síndrome vertiginosa.19
Com relação às disfunções vestibulares estabelecidas, crescem paralela e lentamente as evidências que conectam a transição climatérica, sua manifestação e evolução. Para a doença de Méniere, por exemplo, foram reportados níveis séricos significativamente menores do estradiol em mulheres acometidas quando comparadas com controles pareadas pela idade. Ainda, encontrou-se correlação significativa, ainda que fraca, entre tais índices hormonais e o valor da predominância labiríntica – medida objetiva de assimetria vestibular na doença, obtida entre as pacientes estudadas.20
Similarmente, evidências conectam o climatério e a evolução das disfunções migranosas, como a migrânea vestibular. É sabido que tais condições são mais comuns em mulheres e que a perimenopausa é um período especialmente susceptível à sua manifestação. Além disso, os neuroesteroides ovarianos parecem regular sistemas neurotransmissores e o efeito de moléculas, como o peptídeo relacionado ao gene da calcitonina (CGRP, do termo em inglês), implicados na fisiopatologia dessas disfunções. Com a irregularidade e alargamento dos ciclos menstruais durante o climatério, o período de vulnerabilidade cíclica aos episódios de migrânea estão ampliados.21,22 Pesquisas clínicas começam a reforçar essa associação entre pacientes com migrânea vestibular. Nesse sentido, em pacientes pós-menopausa com a doença, os níveis do estradiol, da progesterona e da testosterona se mostraram significativamente reduzidos em comparação com controles. Além disso, entre pacientes com migrânea vestibular, aquelas com maiores concentrações do estradiol apresentaram menor gravidade do quadro, menor severidade, frequência e duração dos episódios de tontura reportados.23
Investigações em andamento nos serviços de Otoneurologia do Hospital de Clínicas da Universidade Federal do Paraná (HC-UFPR) e no Hospital das Clínicas da Universidade de São Paulo (HC-USP) têm procurado escrutinar as características dos quadros vestibulares episódicos em mulheres climatéricas. Ainda que preliminares, a experiência até o momento aponta para a correlação entre as escalas clínicas vestibulares e aquelas ligadas a esse período da vida da mulher (Figura 3). Tais observações sugerem um reforço indireto do impacto da transição hormonal nas vias vestibulares, e direciona para a existência de marcadores clínicos e laboratoriais para essa relação.
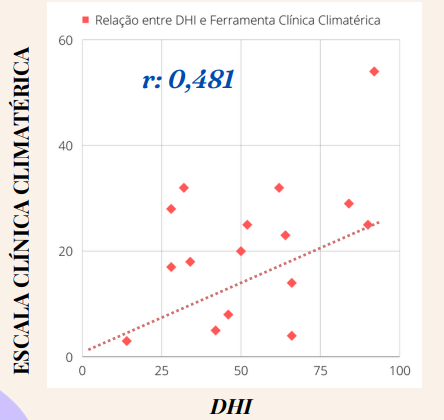
Figura 3: Gráfico de dispersão entre os valores obtidos para a escala clínica de avaliação de queixas vestibulares, Dizziness Handicap Inventory (DHI) e a escala de sintomas climatéricos, entre pacientes sintomáticas. Coeficiente de Pearson (r: 0,481) demonstra moderada correlação entre as variáveis. (Resultados preliminares do ambulatório de estudo de disfunções vestibulares episódicas no climatério, da Universidade Federal do Paraná). Fonte: o Autor.
Em suma, há demonstrações robustas da influência dos hormônios no sistema vestibular ao longo da vida da mulher. O climatério, por sua vez, é um período especialmente vulnerável à manifestação de disfunções neurológicas de ordem diversa, como a tontura. Essa propensão decorre de mecanismos complexos, neuromicroestruturais, bioenergéticos e inflamatórios, que conectam o estradiol ao funcionamento vestibular. Deve-se considerar, contudo, que o período apresenta comumente outras repercussões, como a piora do sono e alterações do humor, que indiretamente poderiam impactar os sistemas vestibular e perceptual. Ainda assim, investigações preliminares indicam repercussões significativas da transição hormonal climatérica em síndromes vestibulares conhecidas, que precisam ser melhor destrinchadas. Estudos em andamento e futuros possibilitarão impulsionar o conhecimento sobre o assunto, fomentar seu reconhecimento pelos profissionais de saúde e apontar caminhos para melhorar a abordagem e tratamento das pacientes com queixas vestibulares nessa fase da vida.
REFERÊNCIAS
AUTORES:
ABSTRACT
Background and purpose: Vertigo and dizziness are common complaints in emergency departments and primary care, and pose major diagnostic challenges due to their various underlying etiologies. Most supportive diagnostic algorithms concentrate on either identifying cerebrovascular events (CVEs) or diagnosing specific vestibular disorders or are restricted to specific patient subgroups. The aim of the present study was to develop and validate a comprehenisve algorithm for identifying patients with CVE and classifying the most common vestibular disorders.
Methods: The study was conducted within the scope of the “PoiSe” project (Prevention, Online feedback, and Interdisciplinary Therapy of Acute Vestibular Syndromes by e-health). A three-level algorithm was developed according to international guidelines and scientific evidence, addressing both the detection of CVEs and the classification of non-vascular vestibular disorders (unilateral vestibulopathy, benign paroxysmal positional vertigo, vestibular paroxysmia, Menière’s disease, vestibular migraine, functional dizziness). The algorithm was validated in a prospectively collected dataset of 407 patients with acute vertigo and dizziness presenting to the Emergency Department at the Ludwig-Maximilian University of Munich.
Results: The algorithm assigned 287 of 407 patients to the correct diagnosis, corresponding to an overall accuracy of 71%. CVEs were identified with high sensitivity of 94%. The six most common vestibular disorders were classified with high specificity, above 95%. Random forest identified presence of a paresis, sensory loss, central ocular motor and vestibular signs (HINTS [head impulse test, nystagmus assessment, and test of skew deviation]), and older age as the most important variables indicating a cerebrovascular event.
Conclusions: The proposed diagnostic algorithm can correctly classify the most common vestibular disorders based on a comprehensive set of key questions and clinical examinations. It is easily applied, not limited to subgroups, and might therefore be transferred to broad clinical settings such as primary healthcare.
Veja o texto completo em: https://onlinelibrary.wiley.com/doi/10.1111/ene.15448
No dia 19 de outubro, tivemos a honra de acompanhar a defesa da Tese de Doutorado de César Bertoldo Garcia.
Entitulado “Tontura cervical proprioceptiva: Efeito do calor induzido por nanotubos de carbono”, esse trabalho representa um grande avanço na Otoneurologia brasileira ao dar destaque a esse tema que vem sendo cada vez mais estudado nos últimos anos.
Parabéns, Dr. César! A equipe de Otoneurologia do Hospital das Clínicas da FMUSP tem muito orgulho de participar dessa vitória!



Nos dias 12 a 14 de setembro de 2022, aconteceu a XIV edição do Curso de Interpretação de Vídeo e Eletrooculografia: Teoria e Prática no Hospital das Clínicas da Faculdade de Medicina da USP.
Foram dois dias de aulas teóricas ministradas pela nossa equipe, incluindo interessantíssimas discussões de casos clínicos. O alunos puderam participar ativamente, opinando e tirando dúvidas.
No terceiro dia, tivemos a parte prática no ambulatório de Otoneurologia do HC-FMUSP, com o acompanhamento da realização de exames nos próprios pacientes do nosso serviço.
Após alguns anos sem o curso presencial por conta da pandemia de Covid-19, finalmente pudemos voltar a receber nossos queridos alunos, e agradecemos a presença dos colegas!
https://youtube.com/shorts/yH2yyFXGQE4?feature=share




{kind=link}
{kind=link}
{kind=link}
{kind=link}